

Protective Effects of Cannabidiol on Lesion-Induced Intervertebral Disc Degeneration
João W. Silveira,1 Ana Carolina Issy,1 Vitor A. Castania,1 Carlos E. G. Salmon,2 Marcello H. Nogueira-Barbosa,3Francisco S. Guimarães,4 Helton L. A. Defino,5 and Elaine Del Bel1,*
Partha Mukhopadhyay, Editor
Published online 2014 Dec 17. doi: 10.1371/journal.pone.0113161
Abstract
Disc degeneration is a multifactorial process that involves hypoxia, inflammation, neoinnervation, accelerated catabolism, and reduction in water and glycosaminoglycan content. Cannabidiol is the main non-psychotropic component of the Cannabis sativa with protective and anti-inflammatory properties. However, possible therapeutic effects of cannabidiol on intervertebral disc degeneration have not been investigated yet. The present study investigated the effects of cannabidiol intradiscal injection in the coccygeal intervertebral disc degeneration induced by the needle puncture model using magnetic resonance imaging (MRI) and histological analyses. Disc injury was induced in the tail of male Wistar rats via a single needle puncture. The discs selected for injury were punctured percutaneously using a 21-gauge needle. MRI and histological evaluation were employed to assess the results. The effects of intradiscal injection of cannabidiol (30, 60 or 120 nmol) injected immediately after lesion were analyzed acutely (2 days) by MRI. The experimental group that received cannabidiol 120 nmol was resubmitted to MRI examination and then to histological analyses 15 days after lesion/cannabidiol injection. The needle puncture produced a significant disc injury detected both by MRI and histological analyses. Cannabidiol significantly attenuated the effects of disc injury induced by the needle puncture. Considering that cannabidiol presents an extremely safe profile and is currently being used clinically, these results suggest that this compound could be useful in the treatment of intervertebral disc degeneration.
Introduction
Intervertebral disc (IVD) degeneration is believed to be the main contributor agent for chronic low back pain. It is a major public health problem with great socioeconomic impact worldwide. IVD degeneration is a multifactorial process characterized by serial progressive changes in the morphology, biochemical components and biomechanical function of the IVD [1], [2].
The IVD is identified as an immune-privileged organ with no access to systemic circulation [3]. However, several pieces of evidence support the prominence of the inflammatory response in the pathogenesis of IVD degeneration [4], [5], [6]. In fact, there is an up-regulation of inflammatory factors that shift homeostasis of the extracellular matrix towards a degenerative and catabolic state, with subsequent breakdown of its components [7], [8]. On the other hand, there is conflicting information regarding the efficacy of intradiscal steroid injections in the treatment of IVD [9], [10], [11], [12]. A clinical study conducted by Buttermman (2004) [13] suggested that intradiscal steroid injections are beneficial for a small number of patients with advanced IVD degeneration. This therapeutic strategy could be more effective in special circumstances in which patients have inflammatory end-plate alterations classified as Modic Type I changes [13], [14].
Cannabidiol (CBD) is the major nonpsychotropic phytocannabinoid of Cannabis sativa (up to 40% of Cannabis extracts). Contrary to most cannabinoids, CBD does not produce psychotomimetic or cognitive effects [15], [16]. Interesting, in the last years it has been suggest that CBD produces a plethora of others pharmacological effects, including antioxidant [17], neuroprotective [18], [19], [20], [21], [22], anti-proliferative [23], [24], anti-anxiety [25], [26], hypnotic and antiepileptic [27], anti-nausea [28], anti-ischemic [29], anti-hyperalgesic [30], and anti-inflammatory [31], [32], [33]. In humans, CBD has been tested in preliminary trials related to diseases such as rheumatoid arthritis [34], [35], multiple sclerosis [36], [37], [38], anxiety [16] and psychosis [39], and shows an extremely safe profile [40], [41]. However, the effects of CBD on the treatment of IVD degeneration have not been investigated yet.
The purpose of this study was to evaluate by magnetic resonance imaging (MRI) and histological analysis the effects of intradiscal injection of CBD in an induced coccygeal disc degeneration model.
Material and Methods
Animals
A total of 19 male Wistar rats (300–350 g) were used in this study. Animals were housed in groups of 4, and kept at a temperature of 23±1°C with a 12 hours light-dark cycle. Food and drinking water were available ad libitum. All experiments were conducted according to the principles and procedures described by the Guidelines for the Care and Use of Mammals in Neuroscience and Behavioural Research (Institute for Laboratory Animal Research, USA) and the Guidelines of the School of Medicine (USP, Brazil), whose Animal Ethics Committee for Animal Experimentation analysed and approved the experimental procedures (protocol number 016/2012).
IVD lesion
The animals were anesthetized with ketamine (50 mg/kg) and xylazine (5 mg/kg), injected intraperitoneally (i.p). The coccygeal intervertebral levels Co6–7, Co7–8, Co8–9 and Co9–10 were selected for the study. The details of the experimental design and the induction of IVD lesion by needle puncture in the tail of Wistar rats have been recently published [42]. This methodology was used here with small modifications. Briefly, two non-contiguous discs Co6–7 and Co8–9 were used to induce disc degeneration by needle puncture. The IVD Co7–8 and Co9–10 remained undisturbed to be used as control levels. The IVD Co9–10 received vehicle injection with a 30-gauge needle. The 21-gauge needle was inserted into Co6–7 and Co8–9 at the level of the annulus fibrosus (AF), crossing the nucleus pulposus (NP) up to the contralateral AF. After full penetration, the needle was rotated 360° twice and held for 30 sec.
Intradiscal Injection of CBD or vehicle
The animals were divided into three sub-groups (with 6–7 animals each) according to CBD doses (Fig. 1). Under general anesthesia, immediately after the disc puncture, 2 µl of CBD (30, 60 or 120 nmol) diluted in 98% saline and 2% Tweem-80 was injected into the Co6–7 lesioned discs. Likewise, the lesioned discs Co8–9 and the non-lesioned discs Co9–10 were injected with vehicle (saline + Tweem-80; 2 µl). Both CBD and vehicle injections were conducted using a Hamilton micro-syringe attached to a 30-gauge needle.
Figure 1
Schematic time line representation of the experimental design.
MRI acquisition
The MRI was performed under general anesthesia 2 and 15 days after the IVD puncture. Images were acquired in a 3.0 T MR scanner (Philips, Achieva, The Netherlands) using a dedicated coil for small animal. The tail was inserted into a tub containing a 0.1 M CuSO4 solution to increase the contrast in the image. A 2-D spin- echo, dual echo sequence was obtained with the following parameters: repetition time = 9000 ms, echo times = 16 (Proton density, PD) and 80 (T2-weigthed) ms, flip angle = 90, numbers of averages = 2, slice thickness = 0,6 mm, field of view = 40×40 mm, in plane resolution = 0.1 mm, 30 sagittal slices. A linear combination of both images (PD and T2) showed excellent anatomical details and it was used to perform a qualitative evaluation of disc integrity. The disc signal intensity was estimated in the T2-weighted image (Echo time = 80 ms) as an indirect measure of disc conditions and its water content. Four discs from Co6–7 to Co9–10 for each animal were analyzed using the Image J software. In order to evaluate the entire disc, five sequential sagittal images were considered and the mean pixel intensity value was quantified.
Histological score
Animals were sacrificed by CO2 inhalation 15 days after the disc puncture. IVDs were removed, fixed in buffered 4% PFA for 24 hours and then subjected to the decalcification process in an ETDA solution consisting of 12% hydrochloric acid, 0.07% EDTA, 0.014% sodium tartrate, 0.8% sodium and potassium tartrate, in water, during 24 hours. After descaling, IVDs were dehydrated, embedded in paraffin and 5 µm sections were obtained with a microtome (Leica RM2145). The sections were then stained with hematoxylin and eosin for histological score and graded by an observer blind to the treatment conditions using the definition established by Norcross et al. 2003 [43], with some modifications (Table 1), under a light microscope (Leica, Germany) at 5× magnification. A grade score ranged from 1 (several degenerated disc) to 5 (normal disc) was assigned separately to both AF and NP.
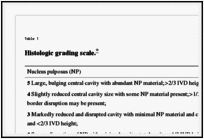
Table 1
Histologic grading scale.*
Statistical Analysis
The MRI data (mean ±SEM; n = 5–7) was analyzed by one-way ANOVA followed by the Newman-Keuls Multiple Comparison Test. The histological scores were analyzed by the non-parametric Kruskal-Wallis test followed by Mann-Whitney and data was represented as the median value. In all cases, the level of significance was set at p<0.05.
Results
Experimental validation: effectiveness of the puncture lesion model
Fig. 2 shows the typical morphology of the intact IVD, which presents an AF with well-organized fibers and a clearly defined border. The NP comprises a significant disc area in the sagittal sections with minimal disruption in its border. Clear histological changes can be observed in the IVD after lesion with the needle puncture. Disc sections showed an AF with lamellar disorganization/fragmentation. NP presented complete obliteration of its cavity with fibrous material. Also, there is a significant decrease of the IVD height.
Figure 2
Representative histological sections of IVD.
The MR images of the NP in the punctured discs showed weaker signal intensities than those of the intact control discs two days after needle puncture. In the NP, decreased water, proteoglycans and increased collagen content are classical technical features of degenerated IVD, which can be visualized on MRI with T2 weighting as a hypointense signal. Representative serial T2-weighted midsagittal images of the intact and punctured tail discs are shown in Fig. 3.
Figure 3
Representative serial T2-weighted midsagittal MRI.
Effects of intradiscal injection of cannabidiol (30, 60 or 120 nmol)
IVD lesion caused significant reduction in the MRI signal intensity two days after the needle puncture. The punctured discs showed a significant decrease in MRI pixel intensity two days after the procedure compared to the intact discs that received or not vehicle injection Co9–10/Co7–8, respectively (Fig. 4 A: [F(3,20) = 27.58, p = 0.0001]; B: [F(3,17) = 9.233, p = 0.0008] and C [F(3,20) = 12.07, p<0.0001]). Vehicle injection per se in the intact discs caused a significant reduction in MRI pixel intensity compared to the non-injected discs in all experimental groups (Fig. 4).

Figure 4
MRI evaluation 2 days after lesion and CBD injection.
Treatment with CBD 30 or 60 nmol immediately after lesion did not modify MRI pixel intensity (Fig. 4A and B). Microinjection of CBD 120 nmol immediately after lesion significantly improved MRI pixel intensity two days after the injection compared to the vehicle injected lesioned discs (Fig. 4C).
Long-term effects of intradiscal injection of cannabidiol (120 nmol)
Fifteen days after the puncture procedure discs which received vehicle injection (Co8–9) showed a significant decrease in MRI pixel intensity compared to the intact disc that received or not a vehicle injection (Co9–10/Co7–8, respectively; [F(3,19) = 14.10, p<0.0001]; Fig. 5).
Figure 5
MRI evaluation 15 days after lesion and CBD injection.
Injection of CBD 120 nmol immediately after lesion significantly improved MRI pixel intensity. The effect was maintained at least for 15 days after injection compared to the vehicle injected lesioned discs (Fig. 5).
MRI data was corroborated by histological results. The histological score was evaluated at fifteen days after the lesion and injection of vehicle or CBD 120. The lesion decreased the histological scores in the AF and NP. CBD 120 nmol prevented the typical histological changes in the AF. No histological changes were observed when the vehicle was injected into the intact disc (Fig. 6).
Figure 6
Effects of CBD on histological scores 15 days after IVD puncture.
Discussion
The primary objective of this study was to investigate the ability of CBD to decrease degenerative events induced by needle puncture of the IVD. Three concentrations of CBD were injected into the IVDs immediately after the disc puncture.
The beneficial effect of CBD, as measured by high resolution MRI, was evaluated two days after the injection in all experimental groups. Only with the concentration of 120 nmol an improvement in the MRI signal intensity was observed. Following this result, an additional analysis was conducted 15 days after CBD 120 nmol injection.
MRI is a non-invasive technique that is the most important method for clinical assessment of IVD pathology. The signal loss on T2-weighted MRIs correlates with the progressive degenerative changes of the IVD [44], [45]. The brightness of the NP has been shown to directly correlate with proteoglycan concentration [46], even more than gross tissue morphology [47]. Higher proteoglycan content in the NP induces water accumulation and increases MRI signal. This region is most severely affected during disc degeneration and, consequently, is a focus for novel cell-based regenerative strategies [48]. However, the 30-gauge needle used for vehicle injection induced significant changes in MRI pixel intensity of the non-puncture discs. Therefore this methodology must be used with considerable caution.
Histological features of the degenerating IVD include specific changes of the NP and AF [43], [49], [50]. The NP shows severe disruption and a gradual decrease in cell number, with reduction in its cavity until complete obliteration. This is consistent with the loss of proteoglycan seen in degenerative models [43], [49], [50] and in human degenerated discs [51]. The AF had radial gaps between lamellae with fragmentation culminating in regions of disorganized fibrous material replacing central lamellae [43], [49], [50]. CBD treatment was able to attenuate the decrease in histological scores induced by the lesion in the AF, but not in the NP region. This lack of correlation between the MRI and histological analysis in the latter region suggest, at least in the present model, a higher sensitivity of the former method.
Multiple mechanisms of action have been proposed to explain CBD effects. It could antagonize the cannabinoids receptors CB1 and CB2 in low nanomolar range and to function as an inverse agonist at 1–10 µM [52]. However, to date, the presence of cannabinoids receptors has not been described in the IVD. CBD also acts as an inhibitor of anandamide uptake and hydrolysis enzymes [53], which results in enhanced levels of this endocannabinoid that might account for the anti-hyperalgesic and anti-inflammatory actions of CBD. Moreover, as a vanilloid receptor agonist with potency equivalent to capsaicin, CBD can desensitize vanilloid receptor 1 and leads to analgesic and anti-inflammatory effects [53]. The competitive inhibition of adenosine uptake and the resulting enhancement of adenosine signaling can also be involved in the anti-inflammatory effects of CBD [54].
Considering that the modulation of immune responses in the degenerate disc is essential for the recovery of this immune-privileged organ [3], [55], the effects of CBD in lesion-induced degeneration could depend on its anti-inflammatory profile. Disc degeneration involves the release of many inflammatory signaling molecules [31], [56], [4], [5], [6]. In most models of inflammation, CBD attenuates inflammatory cell migration/infiltration [57], [33] and the production of inflammatory mediators [58]. For example, CBD suppresses proinflammatory signaling, including NF-κB, induced by LPS [56]. Time- and dose-dependent anti-inflammatory activity has also been observed in acute inflammation models [31]. CBD is also effective in chronic neuropathic painful states that are associated with the release of proinflammatory cytokines, such as IL-6, IL-1β, and TNFα [20], [33], [56]. Moreover, CBD can abolish the increase of nitric oxide levels in paw tissues in inflammatory and neuropathic pain models [59]. Finally, the ability of CBD to reduce inflammatory markers has been shown in several experimental different conditions. CBD treatment inhibits the progression of periodontitis that was accompanied by a decrease in neutrophil migration, expression of bone related molecules and production of IL-1β and TNF-α [33]. In arthritis models, CBD blocks its progression, decreasing collagen II-specific proliferation and IFN-γ production, as well as decreasing the release of TNF-α by synovial cells [35]. In diabetic retina, the increase in phosphorylation of p38 MAP kinase, a stress-activated protein kinase that is a downstream target of proinflammatory cytokines, is blocked by CBD treatment [60]. Additionally, CBD beneficial effects have been recently described in the liver injury model of hepatic ischemia/reperfusion by attenuating inflammatory signaling in a CB1/2 receptors independent manner [61], [62].
In summary our study revealed anti-degenerative effects of intradiscal microinjection of CBD 120 nmol. CBD represents one of the most promising candidates present in the Cannabis sativa plant for clinical use due to its remarkable lack of cognitive or psychotomimetic actions. It has been already approved in several countries for the treatment of neuropathic pain [63]. Although further research is necessary to clarify the mechanisms involved in CBD effects, the present results suggest the possibility of its use for disc degeneration treatment.
Acknowledgments
We would like to thank Célia Ap. da Silva for the technical support and to João Francisco Cordeiro Pedrazzi for his helpful assistance with cannabidiol.
Ethics Committee for Animal Experimentation of the University of São Paulo (CETEA, protocol n° 016/2012).
Funding Statement
This research was supported by CAPES/PNPD, Brazil. The equipment and drugs used in this work were acquired from FAPESP, CNPq, and CAPES, Brazil. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
References
1. Zhang Y, An HS, Tannoury C, Thonar EJ, Freedman MK, et al. (2008) Biological treatment for degenerative disc disease: implications for the field of physical medicine and rehabilitation. Am J Phys Med Rehabil 87:694–702. [PubMed]
2. An HS, Thonar EJ, Masuda K (2003) Biological repair of intervertebral disc Spine. 28:S86–92. [PubMed]
3. Sun Z, Zhang M, Zhao XH, Liu ZH, Gao Y, et al. (2013) Immune cascades in human intervertebral disc: the pros and cons. Int J Clin Exp Pathol. 6:1009–14. [PMC free article] [PubMed]
4. Takahashi H, Suguro T, Okazima Y, Motegi M, Okada Y, et al. (1996) Inflammatory cytokines in the herniated disc of the lumbar spine. Spine 21:218–24. [PubMed]
5. Burke JG, Watson RW, MCcormack D, Dowling FE, Walsh MG, et al. (2002) Intervertebral discs which cause low back pain secrete high levels of proinflammatory mediators. J Bone Joint Surg Br 84:196–201. [PubMed]
6. De Souza Grava AL, Ferrari LF, Defino HL (2012) Cytokine inhibition and time-related influence of inflammatory stimuli on the hyperalgesia induced by the nucleus pulposus. Eur Spine J 21:537–45. [PMC free article] [PubMed]
7. Goldring MB (2000) The role of the chondrocyte in osteoarthritis. Arthritis Rheum 43:1916–26. [PubMed]
8. Lee S, Moon CS, Sul D, Lee J, Bae M, et al. (2009) Comparison of growth factor and cytokine expression in patients with degenerated disc disease and herniated nucleus pulposus. Clin Biochem42:1504–11. [PubMed]
9. Simmons JW, Mcmillin JN, Emery SF, Kimmich SJ (1992) Intradiscal steroids. A prospective double-blind clinical trial. Spine 17:S172–75. [PubMed]
10. Khot A, Bowditch M, Powell J, Sharp D (2004) The use of intradiscal steroid therapy for lumbar spinal discogenic pain: a randomized controlled trial. Spine 29:833–6. [PubMed]
11. Staal JB, De Bie RA, de Vet HC. W Hildebrandt J, Nelemans P (2009) Injection therapy for subacute and chronic low back pain: an updated Cochrane review. Spine 34:49–59. [PubMed]
12. Chou R, Atlas SJ, Stanos SP, Rosenquist RW (2009) Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine 34:1078–93. [PubMed]
13. Butterman GR (2004) The effect of spinal steroid injections for degenerative disc desease. Spine4:495–505. [PubMed]
14. Carragee EJ (2011) Editorial. Intradiscal treatment of back pain. The Spine Journal 11:97–9. [PubMed]
15. Mechoulam R, Peters M, Murillo-Rodriguez E, Hanus LO (2007) Cannabidiol-recent advances. Chem Biodivers 4:1678–92. [PubMed]
16. Izzo AA, Borrelli F, Capasso R, Di Marzo V, Mechoulam R (2009) Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb. Trends Pharmacol Sci 30:515–27. [PubMed]
17. Hampson AJ, Grimaldi M, Axelrod J, Wink D (1998) Cannabidiol and (-) Delta9-tetrahydrocannabinol are neuroprotective antioxidants. Proc Natl Acad Sci USA 95:8268–73. [PMC free article] [PubMed]
18. Esposito G, De Filippis D, Carnuccio R, Izzo AA, Iuvone T (2006) The marijuana component cannabidiol inhibits beta-amyloid-induced tau protein hyperphosphorylation through Wnt/beta-catenin pathway rescue in PC12 cells. J Mol Med (Berl) 84:253–58. [PubMed]
19. Dirikoc S, Priola Sa, Marella M, Zsurger N, Chabry J (2007) Nonpsychoactive cannabidiol prevents prion accumulation and protects neurons against prion toxicity. J Neurosci 27:9537–44. [PubMed]
20. Esposito G, Scuderi C, Savani C, Steardo LJR, de Filippis D, et al. (2007) Cannabidiol in vivo blunts beta-amyloid induced neuroinflammation by suppressing IL-1beta and iNOS expression. Br J Pharmacol151:1272–79. [PMC free article] [PubMed]
21. Kwiatkoski M, Guimarães FS, Del-Bel E (2012) Cannabidiol-treated rats exhibited higher motor score after cryogenic spinal cord injury. Neurotox Res 21:271–80. [PubMed]
22. Perez M, Benitez SU, Cartarozzi LP, Del Bel E, Guimarães FS, et al. (2013) Neuroprotection and reduction of glial reaction by cannabidiol treatment after sciatic nerve transection in neonatal rats. Eur J Neurosci v. 38:3424–34. [PubMed]
23. Ligresti A, Moriello AS, Starowicz K, Matias I, Pisanti S, et al. (2006) Antitumor activity of plant cannabinoids with emphasis on the effect of cannabidiol on human breast carcinoma. J Pharmacol Exp Ther 318:1375–87. [PubMed]
24. Massi P, Valenti M, Vaccani A, Gasperi V, Perletti G, et al. (2008) 5-Lipoxygenase and anandamide hydrolase (FAAH) mediate the antitumor activity of cannabidiol, a non-psychoactive cannabinoid. J Neurochem 104:1091–1100. [PubMed]
25. Guimaraes FS, Chiaretti TM, Graeff FG, Zuardi AW (2006) Antianxiety effect of cannabidiol in the elevated plus-maze. Psychopharmacology (Berl) 100:558–59. [PubMed]
26. Moreira FA, Aguiar DC, Guimaraes FS (2006) Anxiolytic-like effect of cannabidiol in the rat Vogel conflict test. Prog Neuropsychopharmacol Biol Psychiatry 30:1466–71. [PubMed]
27. Carlini EA, Cunha JM (1981) Hypnotic and antiepileptic effects of cannabidiol. J Clin Pharmacol21:417S–427S. [PubMed]
28. Rock EM, Limebeer CL, Mechoulam R, Piomelli D, Parker LA (2008) The effect of cannabidiol and URB597 on conditioned gaping (a model of nausea) elicited by a lithium-paired context in the rat. Psychopharmacology (Berl) 196:389–95. [PubMed]
29. Durst R, Danenberg H, Gallily R, Mechoulam R, Meir K, et al. (2007) Cannabidiol, a nonpsychoactive Cannabis constituent, protects against myocardial ischemic reperfusion injury. Am J Physiol Heart Circ Physiol 293:H3602–07. [PubMed]
30. Costa B, Giagnoni G, Franke C, Trovato AE, Colleoni M (2004) Vanilloid TRPV1 receptor mediates the antihyperalgesic effect of the nonpsychoactive cannabinoid, cannabidiol, in a rat model of acute inflammation. Br J Pharmacol 143:247–50. [PMC free article] [PubMed]
31. Costa B, Colleoni M, Conti S, Parolaro D, Franke C, et al. (2004) Oral anti-inflammatory activity of cannabidiol, a non-psychoactive constituent of cannabis, in acute carrageenan-induced inflammation in the rat paw. Arch Pharmacol 369:294–99. [PubMed]
32. Croxford JL, Yamamura T (2005) Cannabinoids and the immune system: potential for the treatment of inflammatory diseases? J Neuroimmunol 166:3–18. [PubMed]
33. Napimoga MH, Benatti BB, Lima FO, Alves PM, Campos AC, et al. (2009) Cannabidiol decreases bone resorption by inhibiting RANK/RANKL expression and pro-inflammatory cytokines during experimental periodontitis in rats. Int Immunopharmacol 9:216–22. [PubMed]
34. Blake DR, Robson P, Ho M, Jubb RW, Mccabe CS (2006) Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology (Oxford) 45:50–2. [PubMed]
35. Malfait AM, Gallily R, Sumariwalla PF, Malik AS, Andreakos E, et al. (2000) The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen-induced arthritis. Proc Natl Acad Sci USA 97:9561–66. [PMC free article] [PubMed]
36. Zajicek J, Fox P, Sanders H, Wright D, Vickery J, et al. (2003) Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicentre randomised placebo-controlled trial. Lancet 362:1517–26. [PubMed]
37. Brady CM, Dasgupta R, Dalton C, Wiseman OJ, Berkley KJ, et al. (2004) An open-label pilot study of cannabis-based extracts for bladder dysfunction in advanced multiple sclerosis. Mult Scler 10:425–33. [PubMed]
38. Rog DJ, Nurmikko TJ, Friede T, Young CA (2005) Randomized, controlled trial of cannabis-based medicine in central pain in multiple sclerosis. Neurology 65:812–19. [PubMed]
39. Zuardi AW, Crippa JA, Hallak JE, Pinto JP, Chagas MH, et al. (2009) Cannabidiol for the treatment of psychosis in Parkinson's disease. J Psychopharmacol 23:979–83. [PubMed]
40. Cunha JM, Carlini EA, Pereira AE, Ramos OL, Pimentel C, et al. (1980) Chronic administration of cannabidiol to healthy volunteers and epileptic patients. Pharmacology 21:175–85. [PubMed]
41. Mechoulam R, Hanus L (2002) Cannabidiol: an overview of some chemical and pharmacological aspects. Part I: chemical aspects. Chem Phys Lipids 121:35–43. [PubMed]
42. Issy AC, Castania V, Castania M, Salmon CE, Nogueira-Barbosa MH, et al. (2013) Experimental model of intervertebral disc degeneration by needle puncture in Wistar rats. Braz J Med Biol Res 46:235–44. [PMC free article] [PubMed]
43. Norcross JP, Lester GE, Weinhold P, Dahners LE (2003) An in vivo model of degenerative disc disease. J Orthop Res 21:183–188. [PubMed]
44. Schiebler ML, Camerino VJ, Fallon MD, Zlatkin MB, Grenier N, et al. (1991) In vivo and ex vivo magnetic resonance imaging evaluation of early disc degeneration with histopathologic correlation. Spine16:635–640. [PubMed]
45. Modic MT, Masaryk TJ, Ross JS, Carter JR (1988) Imaging of degenerative disc disease. Radiology168:177–186. [PubMed]
46. Pearce RH, Thompson JP, Bebault GM, Flak B (1991) Magnetic resonance imaging reflects the chemical changes of aging degeneration in the human intervertebral disk. J Rheumatol Suppl 27 42–3. [PubMed]
47. Thompson JP, Pearce RH, Ho B (1988) Correlation of gross morphology and chemical composition with magnetic resonance images of human lumbar intervertebral discs. Trans Orthop Res Soc 13:1.
48. Ludwinski FE, Gnanalingham K, Richardson SM, Hoyland JA (2013) Understanding the native nucleus pulposus cell phenotype has important implications for intervertebral disc regeneration strategies. Regenerative Medicine 8:75–87. [PubMed]
49. Han B, Zhu K, Li FC, Xiao YX, Feng J, et al. (2008) A simple disc degeneration model induced by percutaneous needle puncture in the rat tail. Spine 33:1925–34. [PubMed]
50. Wei A, Williams LA, Bhargav D, Shen B, Kishen T, et al. (2009) BMP13 prevents the effects of annular injury in an ovine model. Int J Biol Sci 5:388–96. [PMC free article] [PubMed]
51. Urban JP, Roberts S (2003) Degeneration of the intervertebral disc. Arthritis Res Ther 5:120–30. [PMC free article] [PubMed]
52. Pertwee RG (2008) The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br J Pharmacol 153:199–215. [PMC free article] [PubMed]
53. Bisogno T, Maccarrone M, De Petrocellis L, Jarrahian A, Finazzi-Agro A, et al. (2001) The uptake by cells of 2-arachidonoylglycerol, an endogenous agonist of cannabinoid receptors. Eur J Biochem268:1982–89. [PubMed]
54. Carrier EJ, Auchampach JA, Hillard CJ (2006) Inhibition of an equilibrative nucleoside transporter by cannabidiol: a mechanism of cannabinoid immunosuppression. Proc Natl Acad Sci USA 103:7895–7900. [PMC free article] [PubMed]
55. Sun Z, Liu ZH, Chen YF, Zhang YZ, Wan ZY, et al. (2013) Molecular immunotherapy might shed a light on the treatment strategies for disc degeneration and herniation. Med Hypotheses 81:477–80. [PubMed]
56. Kozela E, Pietr M, Juknat A, Rimmerman N, Levy R, et al. (2010) Cannabinoids Delta(9)-tetrahydrocannabinol and cannabidiol differentially inhibit the lipopolysaccharide-activated NF-kappaB and interferon-beta/STAT proinflammatory pathways in BV-2 microglial cells. J Biol Chem 285:1616–1626. [PMC free article] [PubMed]
57. Mchugh D, Tanner C, Mechoulam R, Pertwee RG, Ross RA (2008) Inhibition of human neutrophil chemotaxis by endogenous cannabinoids and phytocannabinoids: evidence for a site distinct from CB1 and CB2. Mol Pharmacol 73:441–50. [PubMed]
58. Croxford JL, Yamamura T (2005) Cannabinoids and the immune system: potential for the treatment of inflammatory diseases? J Neuroimmunol 166:3–18. [PubMed]
59. Costa B, Trovato AE, Comelli F, Giagnoni G, Colleoni M (2007) The non-psychoactive cannabis constituent cannabidiol is an orally effective therapeutic agent in rat chronic inflammatory and neuropathic pain. Eur J Pharmacol 556:75–83. [PubMed]
60. El-Remessy AB, Al-Shabrawey M, Khalifa Y, Tsai NT, Caldwell RB, et al. (2006) Neuroprotective and blood-retinal barrier-preserving effects of cannabidiol in experimental diabetes. Am J Pathol 168:235–44. [PMC free article] [PubMed]
61. Mukhopadhyay P, Rajesh M, Horváth B, Bátkai S, Park O, et al. (2011) Cannabidiol protects against hepatic ischemia/reperfusion injury by attenuating inflammatory signaling and response, oxidative/nitrative stress, and cell death. Free Radical Biology & Medicine 50:1368–81. [PMC free article] [PubMed]
62. Fouad AA, Jresat I (2011) Therapeutic potential of cannabidiol against ischemia/reperfusion liver injury in rats. European Journal of Pharmacology 670:216–23. [PubMed]
63. Rahn EJ, Hohmann AG (2009) Cannabinoids as pharmacotherapies for neuropathic pain: from the bench to the bedside. Neurotherapeutics 6:713–37. [PMC free article] [PubMed]
João W. Silveira,1 Ana Carolina Issy,1 Vitor A. Castania,1 Carlos E. G. Salmon,2 Marcello H. Nogueira-Barbosa,3Francisco S. Guimarães,4 Helton L. A. Defino,5 and Elaine Del Bel1,*
Partha Mukhopadhyay, Editor
Published online 2014 Dec 17. doi: 10.1371/journal.pone.0113161
Abstract
Disc degeneration is a multifactorial process that involves hypoxia, inflammation, neoinnervation, accelerated catabolism, and reduction in water and glycosaminoglycan content. Cannabidiol is the main non-psychotropic component of the Cannabis sativa with protective and anti-inflammatory properties. However, possible therapeutic effects of cannabidiol on intervertebral disc degeneration have not been investigated yet. The present study investigated the effects of cannabidiol intradiscal injection in the coccygeal intervertebral disc degeneration induced by the needle puncture model using magnetic resonance imaging (MRI) and histological analyses. Disc injury was induced in the tail of male Wistar rats via a single needle puncture. The discs selected for injury were punctured percutaneously using a 21-gauge needle. MRI and histological evaluation were employed to assess the results. The effects of intradiscal injection of cannabidiol (30, 60 or 120 nmol) injected immediately after lesion were analyzed acutely (2 days) by MRI. The experimental group that received cannabidiol 120 nmol was resubmitted to MRI examination and then to histological analyses 15 days after lesion/cannabidiol injection. The needle puncture produced a significant disc injury detected both by MRI and histological analyses. Cannabidiol significantly attenuated the effects of disc injury induced by the needle puncture. Considering that cannabidiol presents an extremely safe profile and is currently being used clinically, these results suggest that this compound could be useful in the treatment of intervertebral disc degeneration.
Introduction
Intervertebral disc (IVD) degeneration is believed to be the main contributor agent for chronic low back pain. It is a major public health problem with great socioeconomic impact worldwide. IVD degeneration is a multifactorial process characterized by serial progressive changes in the morphology, biochemical components and biomechanical function of the IVD [1], [2].
The IVD is identified as an immune-privileged organ with no access to systemic circulation [3]. However, several pieces of evidence support the prominence of the inflammatory response in the pathogenesis of IVD degeneration [4], [5], [6]. In fact, there is an up-regulation of inflammatory factors that shift homeostasis of the extracellular matrix towards a degenerative and catabolic state, with subsequent breakdown of its components [7], [8]. On the other hand, there is conflicting information regarding the efficacy of intradiscal steroid injections in the treatment of IVD [9], [10], [11], [12]. A clinical study conducted by Buttermman (2004) [13] suggested that intradiscal steroid injections are beneficial for a small number of patients with advanced IVD degeneration. This therapeutic strategy could be more effective in special circumstances in which patients have inflammatory end-plate alterations classified as Modic Type I changes [13], [14].
Cannabidiol (CBD) is the major nonpsychotropic phytocannabinoid of Cannabis sativa (up to 40% of Cannabis extracts). Contrary to most cannabinoids, CBD does not produce psychotomimetic or cognitive effects [15], [16]. Interesting, in the last years it has been suggest that CBD produces a plethora of others pharmacological effects, including antioxidant [17], neuroprotective [18], [19], [20], [21], [22], anti-proliferative [23], [24], anti-anxiety [25], [26], hypnotic and antiepileptic [27], anti-nausea [28], anti-ischemic [29], anti-hyperalgesic [30], and anti-inflammatory [31], [32], [33]. In humans, CBD has been tested in preliminary trials related to diseases such as rheumatoid arthritis [34], [35], multiple sclerosis [36], [37], [38], anxiety [16] and psychosis [39], and shows an extremely safe profile [40], [41]. However, the effects of CBD on the treatment of IVD degeneration have not been investigated yet.
The purpose of this study was to evaluate by magnetic resonance imaging (MRI) and histological analysis the effects of intradiscal injection of CBD in an induced coccygeal disc degeneration model.
Material and Methods
Animals
A total of 19 male Wistar rats (300–350 g) were used in this study. Animals were housed in groups of 4, and kept at a temperature of 23±1°C with a 12 hours light-dark cycle. Food and drinking water were available ad libitum. All experiments were conducted according to the principles and procedures described by the Guidelines for the Care and Use of Mammals in Neuroscience and Behavioural Research (Institute for Laboratory Animal Research, USA) and the Guidelines of the School of Medicine (USP, Brazil), whose Animal Ethics Committee for Animal Experimentation analysed and approved the experimental procedures (protocol number 016/2012).
IVD lesion
The animals were anesthetized with ketamine (50 mg/kg) and xylazine (5 mg/kg), injected intraperitoneally (i.p). The coccygeal intervertebral levels Co6–7, Co7–8, Co8–9 and Co9–10 were selected for the study. The details of the experimental design and the induction of IVD lesion by needle puncture in the tail of Wistar rats have been recently published [42]. This methodology was used here with small modifications. Briefly, two non-contiguous discs Co6–7 and Co8–9 were used to induce disc degeneration by needle puncture. The IVD Co7–8 and Co9–10 remained undisturbed to be used as control levels. The IVD Co9–10 received vehicle injection with a 30-gauge needle. The 21-gauge needle was inserted into Co6–7 and Co8–9 at the level of the annulus fibrosus (AF), crossing the nucleus pulposus (NP) up to the contralateral AF. After full penetration, the needle was rotated 360° twice and held for 30 sec.
Intradiscal Injection of CBD or vehicle
The animals were divided into three sub-groups (with 6–7 animals each) according to CBD doses (Fig. 1). Under general anesthesia, immediately after the disc puncture, 2 µl of CBD (30, 60 or 120 nmol) diluted in 98% saline and 2% Tweem-80 was injected into the Co6–7 lesioned discs. Likewise, the lesioned discs Co8–9 and the non-lesioned discs Co9–10 were injected with vehicle (saline + Tweem-80; 2 µl). Both CBD and vehicle injections were conducted using a Hamilton micro-syringe attached to a 30-gauge needle.
Figure 1
Schematic time line representation of the experimental design.
MRI acquisition
The MRI was performed under general anesthesia 2 and 15 days after the IVD puncture. Images were acquired in a 3.0 T MR scanner (Philips, Achieva, The Netherlands) using a dedicated coil for small animal. The tail was inserted into a tub containing a 0.1 M CuSO4 solution to increase the contrast in the image. A 2-D spin- echo, dual echo sequence was obtained with the following parameters: repetition time = 9000 ms, echo times = 16 (Proton density, PD) and 80 (T2-weigthed) ms, flip angle = 90, numbers of averages = 2, slice thickness = 0,6 mm, field of view = 40×40 mm, in plane resolution = 0.1 mm, 30 sagittal slices. A linear combination of both images (PD and T2) showed excellent anatomical details and it was used to perform a qualitative evaluation of disc integrity. The disc signal intensity was estimated in the T2-weighted image (Echo time = 80 ms) as an indirect measure of disc conditions and its water content. Four discs from Co6–7 to Co9–10 for each animal were analyzed using the Image J software. In order to evaluate the entire disc, five sequential sagittal images were considered and the mean pixel intensity value was quantified.
Histological score
Animals were sacrificed by CO2 inhalation 15 days after the disc puncture. IVDs were removed, fixed in buffered 4% PFA for 24 hours and then subjected to the decalcification process in an ETDA solution consisting of 12% hydrochloric acid, 0.07% EDTA, 0.014% sodium tartrate, 0.8% sodium and potassium tartrate, in water, during 24 hours. After descaling, IVDs were dehydrated, embedded in paraffin and 5 µm sections were obtained with a microtome (Leica RM2145). The sections were then stained with hematoxylin and eosin for histological score and graded by an observer blind to the treatment conditions using the definition established by Norcross et al. 2003 [43], with some modifications (Table 1), under a light microscope (Leica, Germany) at 5× magnification. A grade score ranged from 1 (several degenerated disc) to 5 (normal disc) was assigned separately to both AF and NP.
Table 1
Histologic grading scale.*
Statistical Analysis
The MRI data (mean ±SEM; n = 5–7) was analyzed by one-way ANOVA followed by the Newman-Keuls Multiple Comparison Test. The histological scores were analyzed by the non-parametric Kruskal-Wallis test followed by Mann-Whitney and data was represented as the median value. In all cases, the level of significance was set at p<0.05.
Results
Experimental validation: effectiveness of the puncture lesion model
Fig. 2 shows the typical morphology of the intact IVD, which presents an AF with well-organized fibers and a clearly defined border. The NP comprises a significant disc area in the sagittal sections with minimal disruption in its border. Clear histological changes can be observed in the IVD after lesion with the needle puncture. Disc sections showed an AF with lamellar disorganization/fragmentation. NP presented complete obliteration of its cavity with fibrous material. Also, there is a significant decrease of the IVD height.
Figure 2
Representative histological sections of IVD.
The MR images of the NP in the punctured discs showed weaker signal intensities than those of the intact control discs two days after needle puncture. In the NP, decreased water, proteoglycans and increased collagen content are classical technical features of degenerated IVD, which can be visualized on MRI with T2 weighting as a hypointense signal. Representative serial T2-weighted midsagittal images of the intact and punctured tail discs are shown in Fig. 3.
Figure 3
Representative serial T2-weighted midsagittal MRI.
Effects of intradiscal injection of cannabidiol (30, 60 or 120 nmol)
IVD lesion caused significant reduction in the MRI signal intensity two days after the needle puncture. The punctured discs showed a significant decrease in MRI pixel intensity two days after the procedure compared to the intact discs that received or not vehicle injection Co9–10/Co7–8, respectively (Fig. 4 A: [F(3,20) = 27.58, p = 0.0001]; B: [F(3,17) = 9.233, p = 0.0008] and C [F(3,20) = 12.07, p<0.0001]). Vehicle injection per se in the intact discs caused a significant reduction in MRI pixel intensity compared to the non-injected discs in all experimental groups (Fig. 4).
Figure 4
MRI evaluation 2 days after lesion and CBD injection.
Treatment with CBD 30 or 60 nmol immediately after lesion did not modify MRI pixel intensity (Fig. 4A and B). Microinjection of CBD 120 nmol immediately after lesion significantly improved MRI pixel intensity two days after the injection compared to the vehicle injected lesioned discs (Fig. 4C).
Long-term effects of intradiscal injection of cannabidiol (120 nmol)
Fifteen days after the puncture procedure discs which received vehicle injection (Co8–9) showed a significant decrease in MRI pixel intensity compared to the intact disc that received or not a vehicle injection (Co9–10/Co7–8, respectively; [F(3,19) = 14.10, p<0.0001]; Fig. 5).
Figure 5
MRI evaluation 15 days after lesion and CBD injection.
Injection of CBD 120 nmol immediately after lesion significantly improved MRI pixel intensity. The effect was maintained at least for 15 days after injection compared to the vehicle injected lesioned discs (Fig. 5).
MRI data was corroborated by histological results. The histological score was evaluated at fifteen days after the lesion and injection of vehicle or CBD 120. The lesion decreased the histological scores in the AF and NP. CBD 120 nmol prevented the typical histological changes in the AF. No histological changes were observed when the vehicle was injected into the intact disc (Fig. 6).
Figure 6
Effects of CBD on histological scores 15 days after IVD puncture.
Discussion
The primary objective of this study was to investigate the ability of CBD to decrease degenerative events induced by needle puncture of the IVD. Three concentrations of CBD were injected into the IVDs immediately after the disc puncture.
The beneficial effect of CBD, as measured by high resolution MRI, was evaluated two days after the injection in all experimental groups. Only with the concentration of 120 nmol an improvement in the MRI signal intensity was observed. Following this result, an additional analysis was conducted 15 days after CBD 120 nmol injection.
MRI is a non-invasive technique that is the most important method for clinical assessment of IVD pathology. The signal loss on T2-weighted MRIs correlates with the progressive degenerative changes of the IVD [44], [45]. The brightness of the NP has been shown to directly correlate with proteoglycan concentration [46], even more than gross tissue morphology [47]. Higher proteoglycan content in the NP induces water accumulation and increases MRI signal. This region is most severely affected during disc degeneration and, consequently, is a focus for novel cell-based regenerative strategies [48]. However, the 30-gauge needle used for vehicle injection induced significant changes in MRI pixel intensity of the non-puncture discs. Therefore this methodology must be used with considerable caution.
Histological features of the degenerating IVD include specific changes of the NP and AF [43], [49], [50]. The NP shows severe disruption and a gradual decrease in cell number, with reduction in its cavity until complete obliteration. This is consistent with the loss of proteoglycan seen in degenerative models [43], [49], [50] and in human degenerated discs [51]. The AF had radial gaps between lamellae with fragmentation culminating in regions of disorganized fibrous material replacing central lamellae [43], [49], [50]. CBD treatment was able to attenuate the decrease in histological scores induced by the lesion in the AF, but not in the NP region. This lack of correlation between the MRI and histological analysis in the latter region suggest, at least in the present model, a higher sensitivity of the former method.
Multiple mechanisms of action have been proposed to explain CBD effects. It could antagonize the cannabinoids receptors CB1 and CB2 in low nanomolar range and to function as an inverse agonist at 1–10 µM [52]. However, to date, the presence of cannabinoids receptors has not been described in the IVD. CBD also acts as an inhibitor of anandamide uptake and hydrolysis enzymes [53], which results in enhanced levels of this endocannabinoid that might account for the anti-hyperalgesic and anti-inflammatory actions of CBD. Moreover, as a vanilloid receptor agonist with potency equivalent to capsaicin, CBD can desensitize vanilloid receptor 1 and leads to analgesic and anti-inflammatory effects [53]. The competitive inhibition of adenosine uptake and the resulting enhancement of adenosine signaling can also be involved in the anti-inflammatory effects of CBD [54].
Considering that the modulation of immune responses in the degenerate disc is essential for the recovery of this immune-privileged organ [3], [55], the effects of CBD in lesion-induced degeneration could depend on its anti-inflammatory profile. Disc degeneration involves the release of many inflammatory signaling molecules [31], [56], [4], [5], [6]. In most models of inflammation, CBD attenuates inflammatory cell migration/infiltration [57], [33] and the production of inflammatory mediators [58]. For example, CBD suppresses proinflammatory signaling, including NF-κB, induced by LPS [56]. Time- and dose-dependent anti-inflammatory activity has also been observed in acute inflammation models [31]. CBD is also effective in chronic neuropathic painful states that are associated with the release of proinflammatory cytokines, such as IL-6, IL-1β, and TNFα [20], [33], [56]. Moreover, CBD can abolish the increase of nitric oxide levels in paw tissues in inflammatory and neuropathic pain models [59]. Finally, the ability of CBD to reduce inflammatory markers has been shown in several experimental different conditions. CBD treatment inhibits the progression of periodontitis that was accompanied by a decrease in neutrophil migration, expression of bone related molecules and production of IL-1β and TNF-α [33]. In arthritis models, CBD blocks its progression, decreasing collagen II-specific proliferation and IFN-γ production, as well as decreasing the release of TNF-α by synovial cells [35]. In diabetic retina, the increase in phosphorylation of p38 MAP kinase, a stress-activated protein kinase that is a downstream target of proinflammatory cytokines, is blocked by CBD treatment [60]. Additionally, CBD beneficial effects have been recently described in the liver injury model of hepatic ischemia/reperfusion by attenuating inflammatory signaling in a CB1/2 receptors independent manner [61], [62].
In summary our study revealed anti-degenerative effects of intradiscal microinjection of CBD 120 nmol. CBD represents one of the most promising candidates present in the Cannabis sativa plant for clinical use due to its remarkable lack of cognitive or psychotomimetic actions. It has been already approved in several countries for the treatment of neuropathic pain [63]. Although further research is necessary to clarify the mechanisms involved in CBD effects, the present results suggest the possibility of its use for disc degeneration treatment.
Acknowledgments
We would like to thank Célia Ap. da Silva for the technical support and to João Francisco Cordeiro Pedrazzi for his helpful assistance with cannabidiol.
Ethics Committee for Animal Experimentation of the University of São Paulo (CETEA, protocol n° 016/2012).
Funding Statement
This research was supported by CAPES/PNPD, Brazil. The equipment and drugs used in this work were acquired from FAPESP, CNPq, and CAPES, Brazil. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
References
1. Zhang Y, An HS, Tannoury C, Thonar EJ, Freedman MK, et al. (2008) Biological treatment for degenerative disc disease: implications for the field of physical medicine and rehabilitation. Am J Phys Med Rehabil 87:694–702. [PubMed]
2. An HS, Thonar EJ, Masuda K (2003) Biological repair of intervertebral disc Spine. 28:S86–92. [PubMed]
3. Sun Z, Zhang M, Zhao XH, Liu ZH, Gao Y, et al. (2013) Immune cascades in human intervertebral disc: the pros and cons. Int J Clin Exp Pathol. 6:1009–14. [PMC free article] [PubMed]
4. Takahashi H, Suguro T, Okazima Y, Motegi M, Okada Y, et al. (1996) Inflammatory cytokines in the herniated disc of the lumbar spine. Spine 21:218–24. [PubMed]
5. Burke JG, Watson RW, MCcormack D, Dowling FE, Walsh MG, et al. (2002) Intervertebral discs which cause low back pain secrete high levels of proinflammatory mediators. J Bone Joint Surg Br 84:196–201. [PubMed]
6. De Souza Grava AL, Ferrari LF, Defino HL (2012) Cytokine inhibition and time-related influence of inflammatory stimuli on the hyperalgesia induced by the nucleus pulposus. Eur Spine J 21:537–45. [PMC free article] [PubMed]
7. Goldring MB (2000) The role of the chondrocyte in osteoarthritis. Arthritis Rheum 43:1916–26. [PubMed]
8. Lee S, Moon CS, Sul D, Lee J, Bae M, et al. (2009) Comparison of growth factor and cytokine expression in patients with degenerated disc disease and herniated nucleus pulposus. Clin Biochem42:1504–11. [PubMed]
9. Simmons JW, Mcmillin JN, Emery SF, Kimmich SJ (1992) Intradiscal steroids. A prospective double-blind clinical trial. Spine 17:S172–75. [PubMed]
10. Khot A, Bowditch M, Powell J, Sharp D (2004) The use of intradiscal steroid therapy for lumbar spinal discogenic pain: a randomized controlled trial. Spine 29:833–6. [PubMed]
11. Staal JB, De Bie RA, de Vet HC. W Hildebrandt J, Nelemans P (2009) Injection therapy for subacute and chronic low back pain: an updated Cochrane review. Spine 34:49–59. [PubMed]
12. Chou R, Atlas SJ, Stanos SP, Rosenquist RW (2009) Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine 34:1078–93. [PubMed]
13. Butterman GR (2004) The effect of spinal steroid injections for degenerative disc desease. Spine4:495–505. [PubMed]
14. Carragee EJ (2011) Editorial. Intradiscal treatment of back pain. The Spine Journal 11:97–9. [PubMed]
15. Mechoulam R, Peters M, Murillo-Rodriguez E, Hanus LO (2007) Cannabidiol-recent advances. Chem Biodivers 4:1678–92. [PubMed]
16. Izzo AA, Borrelli F, Capasso R, Di Marzo V, Mechoulam R (2009) Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb. Trends Pharmacol Sci 30:515–27. [PubMed]
17. Hampson AJ, Grimaldi M, Axelrod J, Wink D (1998) Cannabidiol and (-) Delta9-tetrahydrocannabinol are neuroprotective antioxidants. Proc Natl Acad Sci USA 95:8268–73. [PMC free article] [PubMed]
18. Esposito G, De Filippis D, Carnuccio R, Izzo AA, Iuvone T (2006) The marijuana component cannabidiol inhibits beta-amyloid-induced tau protein hyperphosphorylation through Wnt/beta-catenin pathway rescue in PC12 cells. J Mol Med (Berl) 84:253–58. [PubMed]
19. Dirikoc S, Priola Sa, Marella M, Zsurger N, Chabry J (2007) Nonpsychoactive cannabidiol prevents prion accumulation and protects neurons against prion toxicity. J Neurosci 27:9537–44. [PubMed]
20. Esposito G, Scuderi C, Savani C, Steardo LJR, de Filippis D, et al. (2007) Cannabidiol in vivo blunts beta-amyloid induced neuroinflammation by suppressing IL-1beta and iNOS expression. Br J Pharmacol151:1272–79. [PMC free article] [PubMed]
21. Kwiatkoski M, Guimarães FS, Del-Bel E (2012) Cannabidiol-treated rats exhibited higher motor score after cryogenic spinal cord injury. Neurotox Res 21:271–80. [PubMed]
22. Perez M, Benitez SU, Cartarozzi LP, Del Bel E, Guimarães FS, et al. (2013) Neuroprotection and reduction of glial reaction by cannabidiol treatment after sciatic nerve transection in neonatal rats. Eur J Neurosci v. 38:3424–34. [PubMed]
23. Ligresti A, Moriello AS, Starowicz K, Matias I, Pisanti S, et al. (2006) Antitumor activity of plant cannabinoids with emphasis on the effect of cannabidiol on human breast carcinoma. J Pharmacol Exp Ther 318:1375–87. [PubMed]
24. Massi P, Valenti M, Vaccani A, Gasperi V, Perletti G, et al. (2008) 5-Lipoxygenase and anandamide hydrolase (FAAH) mediate the antitumor activity of cannabidiol, a non-psychoactive cannabinoid. J Neurochem 104:1091–1100. [PubMed]
25. Guimaraes FS, Chiaretti TM, Graeff FG, Zuardi AW (2006) Antianxiety effect of cannabidiol in the elevated plus-maze. Psychopharmacology (Berl) 100:558–59. [PubMed]
26. Moreira FA, Aguiar DC, Guimaraes FS (2006) Anxiolytic-like effect of cannabidiol in the rat Vogel conflict test. Prog Neuropsychopharmacol Biol Psychiatry 30:1466–71. [PubMed]
27. Carlini EA, Cunha JM (1981) Hypnotic and antiepileptic effects of cannabidiol. J Clin Pharmacol21:417S–427S. [PubMed]
28. Rock EM, Limebeer CL, Mechoulam R, Piomelli D, Parker LA (2008) The effect of cannabidiol and URB597 on conditioned gaping (a model of nausea) elicited by a lithium-paired context in the rat. Psychopharmacology (Berl) 196:389–95. [PubMed]
29. Durst R, Danenberg H, Gallily R, Mechoulam R, Meir K, et al. (2007) Cannabidiol, a nonpsychoactive Cannabis constituent, protects against myocardial ischemic reperfusion injury. Am J Physiol Heart Circ Physiol 293:H3602–07. [PubMed]
30. Costa B, Giagnoni G, Franke C, Trovato AE, Colleoni M (2004) Vanilloid TRPV1 receptor mediates the antihyperalgesic effect of the nonpsychoactive cannabinoid, cannabidiol, in a rat model of acute inflammation. Br J Pharmacol 143:247–50. [PMC free article] [PubMed]
31. Costa B, Colleoni M, Conti S, Parolaro D, Franke C, et al. (2004) Oral anti-inflammatory activity of cannabidiol, a non-psychoactive constituent of cannabis, in acute carrageenan-induced inflammation in the rat paw. Arch Pharmacol 369:294–99. [PubMed]
32. Croxford JL, Yamamura T (2005) Cannabinoids and the immune system: potential for the treatment of inflammatory diseases? J Neuroimmunol 166:3–18. [PubMed]
33. Napimoga MH, Benatti BB, Lima FO, Alves PM, Campos AC, et al. (2009) Cannabidiol decreases bone resorption by inhibiting RANK/RANKL expression and pro-inflammatory cytokines during experimental periodontitis in rats. Int Immunopharmacol 9:216–22. [PubMed]
34. Blake DR, Robson P, Ho M, Jubb RW, Mccabe CS (2006) Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology (Oxford) 45:50–2. [PubMed]
35. Malfait AM, Gallily R, Sumariwalla PF, Malik AS, Andreakos E, et al. (2000) The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen-induced arthritis. Proc Natl Acad Sci USA 97:9561–66. [PMC free article] [PubMed]
36. Zajicek J, Fox P, Sanders H, Wright D, Vickery J, et al. (2003) Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicentre randomised placebo-controlled trial. Lancet 362:1517–26. [PubMed]
37. Brady CM, Dasgupta R, Dalton C, Wiseman OJ, Berkley KJ, et al. (2004) An open-label pilot study of cannabis-based extracts for bladder dysfunction in advanced multiple sclerosis. Mult Scler 10:425–33. [PubMed]
38. Rog DJ, Nurmikko TJ, Friede T, Young CA (2005) Randomized, controlled trial of cannabis-based medicine in central pain in multiple sclerosis. Neurology 65:812–19. [PubMed]
39. Zuardi AW, Crippa JA, Hallak JE, Pinto JP, Chagas MH, et al. (2009) Cannabidiol for the treatment of psychosis in Parkinson's disease. J Psychopharmacol 23:979–83. [PubMed]
40. Cunha JM, Carlini EA, Pereira AE, Ramos OL, Pimentel C, et al. (1980) Chronic administration of cannabidiol to healthy volunteers and epileptic patients. Pharmacology 21:175–85. [PubMed]
41. Mechoulam R, Hanus L (2002) Cannabidiol: an overview of some chemical and pharmacological aspects. Part I: chemical aspects. Chem Phys Lipids 121:35–43. [PubMed]
42. Issy AC, Castania V, Castania M, Salmon CE, Nogueira-Barbosa MH, et al. (2013) Experimental model of intervertebral disc degeneration by needle puncture in Wistar rats. Braz J Med Biol Res 46:235–44. [PMC free article] [PubMed]
43. Norcross JP, Lester GE, Weinhold P, Dahners LE (2003) An in vivo model of degenerative disc disease. J Orthop Res 21:183–188. [PubMed]
44. Schiebler ML, Camerino VJ, Fallon MD, Zlatkin MB, Grenier N, et al. (1991) In vivo and ex vivo magnetic resonance imaging evaluation of early disc degeneration with histopathologic correlation. Spine16:635–640. [PubMed]
45. Modic MT, Masaryk TJ, Ross JS, Carter JR (1988) Imaging of degenerative disc disease. Radiology168:177–186. [PubMed]
46. Pearce RH, Thompson JP, Bebault GM, Flak B (1991) Magnetic resonance imaging reflects the chemical changes of aging degeneration in the human intervertebral disk. J Rheumatol Suppl 27 42–3. [PubMed]
47. Thompson JP, Pearce RH, Ho B (1988) Correlation of gross morphology and chemical composition with magnetic resonance images of human lumbar intervertebral discs. Trans Orthop Res Soc 13:1.
48. Ludwinski FE, Gnanalingham K, Richardson SM, Hoyland JA (2013) Understanding the native nucleus pulposus cell phenotype has important implications for intervertebral disc regeneration strategies. Regenerative Medicine 8:75–87. [PubMed]
49. Han B, Zhu K, Li FC, Xiao YX, Feng J, et al. (2008) A simple disc degeneration model induced by percutaneous needle puncture in the rat tail. Spine 33:1925–34. [PubMed]
50. Wei A, Williams LA, Bhargav D, Shen B, Kishen T, et al. (2009) BMP13 prevents the effects of annular injury in an ovine model. Int J Biol Sci 5:388–96. [PMC free article] [PubMed]
51. Urban JP, Roberts S (2003) Degeneration of the intervertebral disc. Arthritis Res Ther 5:120–30. [PMC free article] [PubMed]
52. Pertwee RG (2008) The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br J Pharmacol 153:199–215. [PMC free article] [PubMed]
53. Bisogno T, Maccarrone M, De Petrocellis L, Jarrahian A, Finazzi-Agro A, et al. (2001) The uptake by cells of 2-arachidonoylglycerol, an endogenous agonist of cannabinoid receptors. Eur J Biochem268:1982–89. [PubMed]
54. Carrier EJ, Auchampach JA, Hillard CJ (2006) Inhibition of an equilibrative nucleoside transporter by cannabidiol: a mechanism of cannabinoid immunosuppression. Proc Natl Acad Sci USA 103:7895–7900. [PMC free article] [PubMed]
55. Sun Z, Liu ZH, Chen YF, Zhang YZ, Wan ZY, et al. (2013) Molecular immunotherapy might shed a light on the treatment strategies for disc degeneration and herniation. Med Hypotheses 81:477–80. [PubMed]
56. Kozela E, Pietr M, Juknat A, Rimmerman N, Levy R, et al. (2010) Cannabinoids Delta(9)-tetrahydrocannabinol and cannabidiol differentially inhibit the lipopolysaccharide-activated NF-kappaB and interferon-beta/STAT proinflammatory pathways in BV-2 microglial cells. J Biol Chem 285:1616–1626. [PMC free article] [PubMed]
57. Mchugh D, Tanner C, Mechoulam R, Pertwee RG, Ross RA (2008) Inhibition of human neutrophil chemotaxis by endogenous cannabinoids and phytocannabinoids: evidence for a site distinct from CB1 and CB2. Mol Pharmacol 73:441–50. [PubMed]
58. Croxford JL, Yamamura T (2005) Cannabinoids and the immune system: potential for the treatment of inflammatory diseases? J Neuroimmunol 166:3–18. [PubMed]
59. Costa B, Trovato AE, Comelli F, Giagnoni G, Colleoni M (2007) The non-psychoactive cannabis constituent cannabidiol is an orally effective therapeutic agent in rat chronic inflammatory and neuropathic pain. Eur J Pharmacol 556:75–83. [PubMed]
60. El-Remessy AB, Al-Shabrawey M, Khalifa Y, Tsai NT, Caldwell RB, et al. (2006) Neuroprotective and blood-retinal barrier-preserving effects of cannabidiol in experimental diabetes. Am J Pathol 168:235–44. [PMC free article] [PubMed]
61. Mukhopadhyay P, Rajesh M, Horváth B, Bátkai S, Park O, et al. (2011) Cannabidiol protects against hepatic ischemia/reperfusion injury by attenuating inflammatory signaling and response, oxidative/nitrative stress, and cell death. Free Radical Biology & Medicine 50:1368–81. [PMC free article] [PubMed]
62. Fouad AA, Jresat I (2011) Therapeutic potential of cannabidiol against ischemia/reperfusion liver injury in rats. European Journal of Pharmacology 670:216–23. [PubMed]
63. Rahn EJ, Hohmann AG (2009) Cannabinoids as pharmacotherapies for neuropathic pain: from the bench to the bedside. Neurotherapeutics 6:713–37. [PMC free article] [PubMed]