Its all too stupid for words.
America Is Giving Away the $30 Billion Medical Marijuana Industry
Why? Because the feds are bogarting the weed, while Israel and Canada are grabbing market share.
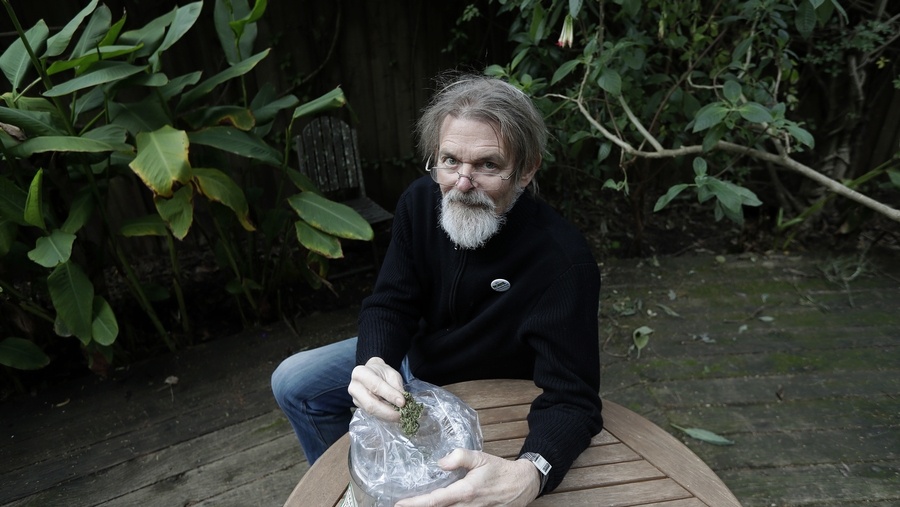
Lyle Craker is an unlikely advocate for any political cause, let alone one as touchy as marijuana law, and that’s precisely why Rick Doblin sought him out almost two decades ago. Craker, Doblin likes to say, is the perfect flag bearer for the cause of medical marijuana production—not remotely controversial and thus the ideal partner in a long and frustrating effort to loosen the Drug Enforcement Administration’s chokehold on cannabis research. There are no counterculture skeletons in Craker’s closet; only dirty boots and botany books. He’s never smoked pot in his life, nor has he tasted liquor. “I have Coca-Cola every once in a while,” says the quiet, white-haired Craker, from a rolling chair in his basement office at the University of Massachusetts at Amherst, where he’s served as a professor in the
Stockbridge School of Agriculture since 1967, specializing in medicinal and aromatic plants. He and his students do things such as subject basil plants to high temperatures to study the effects of climate change on what plant people call the constituents, or active elements.
Craker first applied for a license to grow marijuana for medicinal research in 2001, at the urging of Doblin, the founder and executive director of the
Multidisciplinary Association for Psychedelic Studies (MAPS), a nonprofit that advocates for research on therapeutic uses for LSD, MDMA (aka Ecstasy), marijuana, and other psychedelic drugs. Doblin, who has a doctorate in public policy, makes no secret of his own
prior drug use. He’s been lobbying since the 1980s for federal approval for clinical research trials on various psychedelics, and he saw marijuana as both a promising potential medicine and an important front in the public-relations war. Since 1970 marijuana has been a DEA Schedule I substance, meaning that in the view of the federal government, it’s as
dangerous as LSD, heroin, and Ecstasy, and has “no currently accepted medical use and a high potential for abuse.”
Rick Doblin, relentless advocate.
Photographer: Jonathan Schoonover for Bloomberg Businessweek
By that definition, pot—
now legal for medicinal use by prescription in 29 states and for recreational use in eight—is more dangerous and less efficacious in the federal government’s estimation than cocaine, oxycodone, or methamphetamine, all of which are classified Schedule II. Scientists and physicians are free to apply to the
Food and Drug Administration and
DEA for trials on Schedule I substances, and there are labs with licenses to produce LSD and Ecstasy for that purpose, but anyone who seeks to do FDA-approved research with marijuana is forced to obtain the plants from a single source: Uncle Sam. Specifically, since 1968 the DEA has allowed only one facility to legally cultivate marijuana for research studies, on a 10-acre plot at the University of Mississippi, funded by the National Institute on Drug Abuse and managed by the
Ole Miss School of Pharmacy.
The NIDA license, Doblin says, is a “monopoly” on the supply and has starved legitimate research toward understanding cannabinoids, terpenes, and other constituents of marijuana that seem to quell pain, stimulate hunger, and perhaps even fight cancer. Twice in the late 1990s, Doblin provided funding, PR, and lobbying support for physicians who wanted to study marijuana—one sought a treatment for AIDS-related wasting syndrome, the other wanted to see if it helped migraines—and was so frustrated by the experience that he vowed to break the monopoly. That’s what led him to Craker.
In June 2001, Craker filed an
application for a license to cultivate “research-grade” marijuana at UMass, with the goal of staging FDA-approved studies. Six months later he was told his application had been lost. He reapplied in 2002 and then, after an additional two years of no action, sued the DEA, backed by MAPS. By this point, both U.S. senators from Massachusetts had publicly supported his application, and a federal court of appeals ordered the DEA to respond, which it finally did, denying the application in 2004.
Craker appealed that decision with backing from a powerful bench of allies, including 40 members of Congress, and finally, in February 2007, a DEA administrative law judge ruled that his application for a license should be granted. The decision was not binding, however; it was merely a recommendation to the DEA leadership. Almost two years later, in the last week of the Bush administration, the application was rejected. Craker threw up his hands. He firmly believed marijuana should be more widely grown and studied, but he’d lost any hope that it would happen in his lifetime. And he had basil to attend to.
Then, in August 2016, during the final months of the Obama presidency, the DEA reversed course. It announced that, for the first time in a half-century, it would
grant new licenses.
Doblin, who has seemingly endless supplies of optimism and enthusiasm, convinced the professor there was hope—again. So Craker submitted paperwork, again, along with 25 other groups. The university’s provost co-signed his application, and Senator Elizabeth Warren (D–Mass.) wrote a letter to the DEA in support of his effort.
He’s still waiting to hear back. “I’m never gonna get the license,” Craker says.
Pessimism isn’t surprising from a man who’s been making a reasonable case for 17 years to no avail. Studies around the world have shown that marijuana has considerable promise as a medicine. Craker says he spoke late last year at a hospital in New Hampshire where certain cannabinoids were shown to facilitate healing in brain-damaged mice. “And I thought, ‘If cannabinoids could do that, let’s put them in medicines!’ ” He sighs. “We can’t do the research.”
Another sigh. “I’m naive about a lot about things,” he says. “But it seems to me that we should be looking at cannabis. I mean, if it’s going to kill people, let’s know that and get rid of it. If it’s going to help people, let’s know that and expand on it. … But there’s just something wrong with the DEA. I don’t know what else to say. … Somehow, marijuana’s got a bad name. And it’s tough to let go of.”
Craker looks over some of the plants used in studies in the agriculture department’s greenhouse at UMass.
Photographer: Jonathan Schoonover for Bloomberg Businessweek
Back in 1990, Ethan Russo was a practicing neurologist who’d grown frustrated with his pharmaceutical options. “It occurred to me I was giving increasingly toxic drugs to my patients with less and less benefit,” says Russo, now one of the world’s
leading experts and advocates for research in marijuana medicine. “It caused me to go back to a childhood interest in medicinal plants and see if there were alternatives.”
In 1996, when California became the first state to allow the use of marijuana by prescription, Russo saw an opening. With the support of—who else—Doblin and MAPS, he wrote a protocol and prepared for what he hoped would be a formal clinical trial using cannabis to treat migraines. Obviously, he’d need to use NIDA-supplied marijuana. You can’t do research acceptable to the FDA with marijuana grown illegally, as is all marijuana not grown at Ole Miss.
NIDA twice rejected his applications to use its pot, but then the FDA assumed oversight of what it calls “investigational new drug” applications, and Russo got his approval. In the eyes of the FDA, his study was promising enough to warrant a clinical trial. “With any other drug, I would have been able to begin work on the trial the next day,” he says. But the use of cannabis, and only cannabis, required a second “public health service review,” according to a rule instituted in 1998 to, ostensibly, facilitate more research. In reality, it did the opposite. NIDA denied Russo access to its cannabis. “Despite the fact that the FDA had approved it,” he says.
Around the world, cannabis research was a growing field. Russo began to write and publish on the subject, and in 1998 he was recruited as a consultant by a British startup,
GW Pharmaceuticals Plc, founded by two physicians who’d been granted a license to cultivate cannabis by the U.K. Home Office, which oversees, among other things, security and drug policy.
In 2003, Russo joined GW full time, serving as medical monitor of clinical trials for two drugs developed from marijuana that GW grew: Sativex, for pain caused by cancer, and Epidiolex, for the treatment of severe seizure disorders. Phase III trials for both drugs were conducted in multiple countries, including the U.S. (The FDA doesn’t have a problem with drugs derived from legal pot. It’s just that in the U.S., the only federally legal pot is from Ole Miss.) Sativex is now available in every country in which trials were conducted except the U.S., where GW expects approval soon. “Basically, I had begun working for a foreign company because of the impossibility of doing clinical work with cannabis in the United States,” Russo says. “And here we had a situation where a medicine, made from cannabis, that was manufactured in England, was able to be imported and tested. It was legally impossible to do the same thing based in the U.S.” GW has a market value of more than $2 billion and a robust drug development pipeline.
Doblin’s ultimate goal isn’t to compete with GW Pharmaceuticals. Should the NIDA monopoly ever end, he says, a number of companies will surely want to grow marijuana “to make extracts in nonsmoking delivery systems that can be patented”—that is, pharmaceuticals. This is a good thing, in his estimation. “But MAPS is focused on developing a low-cost generic plant in bud form,” he says. In other words, he wants specific varieties of marijuana, not derivatives thereof, to be FDA-approved.
Many people expect the Republican-controlled Congress to follow its recent tax overhaul by looking for ways to slash costs in Medicaid and Medicare. Legitimate research into the medicinal properties of marijuana could help. Studies show that opioid use drops significantly in states where marijuana has been legalized; this suggests people are consuming the plant for pain, something they could be doing more effectively if physicians and the FDA controlled chemical makeup and potency. A study published in July 2016 in
Health Affairs showed that the use of prescription drugs for which marijuana could serve as a clinical alternative “fell significantly,” saving hundreds of millions of dollars among users of Medicare Part D.
“The marijuana plant in bud form, if we can get it available by the FDA, is going to be incredibly cheap,” Doblin says. His Israeli partners, Better by Cann Pharmaceuticals, can produce organic, high-potency trimmed marijuana for roughly 65¢ a gram, or $18 or so per ounce. “When you’re talking about kicking people off of health insurance and reducing Medicare and Medicaid costs, we better find a way to provide medical relief to people at a low cost,” he says.
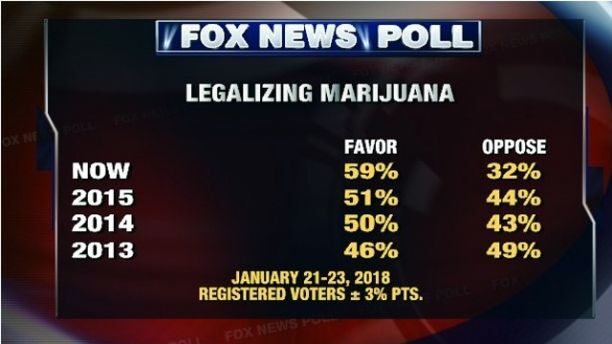
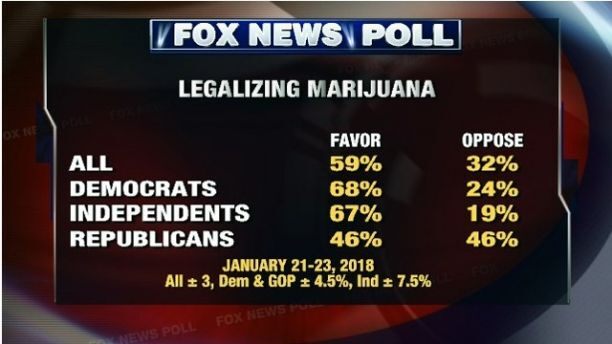
Every year the percentage of Americans who favor legalization of marijuana climbs. Last year it topped 60 percent for the first time. A remarkable 94 percent support medical use. “And businesses outside of the country are already making billions of dollars,” Doblin says. Canada, the Netherlands, and Israel all have booming cannabis research sectors; in Israel, some of the work is government-funded. “We have enormous opportunity that we’re squandering as a country to reduce health-care costs, build businesses, and create jobs,” he says.
Russo agrees. He now lives in Washington state consulting for several biotech startups working on cannabis projects. “Let’s face facts: This is a very technologically advanced nation with a great deal of talent. There is no way, shape, or form that the dangers of cannabis warrant this kind of control,” he says. “There are issues. There are side effects. Anyone who tells you differently is simply inaccurate. However, the kinds of problems related to cannabis administration are totally controllable. And it is a much safer drug than many, if not most, pharmaceuticals that are currently being approved.”
He’d just returned from an industry conference in Medellín, Colombia. “I think that there’s a greater chance of significant clinical cannabis research coming out of Colombia in the coming years than there is in the U.S.,” Russo says. “Why would people allow this loss of business in a situation where, clearly, Americans could be preeminent?”
It’s Happening Without Us, Man
$31 billion: Potential size of global medical cannabis market by 2021
$1 billion: Value of medical cannabis that could be exported annually by Israeli companies
$100 million: Foreign investment in Israeli cannabis startups in 2016
70+ Canadian companies with licenses to cultivate, produce, and sell medical marijuana
Among those who’ve advised Craker is Tony Coulson, a former DEA agent who retired in 2010 and works as a consultant for companies developing drugs. Coulson was vehemently antimarijuana until his son, a combat soldier, came home from the Middle East with post-traumatic stress disorder and needed help. “For years I was of the belief that the science doesn’t say that this is medicine,” he says. “But when you get into this curious history, you find the science doesn’t show it primarily because we’re standing in the way. The NIDA monopoly prevents anyone from getting into further studies.”
Coulson blames the Obama administration for not acting sooner, creating a situation in which the decision on granting new growing licenses was passed down to Attorney General Jeff Sessions, who has publicly declared his belief in the dangers of marijuana. The NIDA monopoly is now his to change. “Sessions has a 1930s
Reefer Madness view of the marijuana world,” Coulson says. “It’s not realistic, and it’s not what rank-and-file DEA really are concerned about. DEA folks have moved beyond this.”
“I guess I take a nationalist approach here,” says Rick Kimball, a former investment banker who’s raising money for a marijuana-related private equity fund and is a trustee for marijuana policy at the Brookings Institution. “We have a huge opportunity in the U.S.,” he says, “and we ought to get our act together. I’m worried that we’re ceding this whole market to the Israelis.”
From left: Craker in his lab; inspecting samples of grass being grown in a cooler.
Photographer: Jonathan Schoonover for Bloomberg Businessweek
Which doesn’t mean there’s no intellectual property left to grab. Research into the chemical makeup of marijuana is still new, but there are at least 160 cannabinoids and as many as 500 terpenes and flavonoids in the plant, all of which can be separated out, mixed, and matched. CBN is thought to aid sleep. CBG may have anticancer potential. One Israeli researcher has synthesized 22 different versions of THC to treat specific neurological conditions. “There’s reason to believe there’s a cornucopia of medicines in there,” Kimball says—medicines that, in theory, are patentable.
At foreign labs, and even at state-licensed operations in Colorado and Washington, plant scientists are growing genetically modified varieties that optimize for certain properties. The majority of their work is focused on increasing potency for recreational use—getting people high—but these companies are learning how to cultivate and engineer plants using increasingly sophisticated methods.
Meanwhile, Mahmoud ElSohly, director of the Marijuana Project at Ole Miss, is growing limited varieties, outdoors, while trying to keep undergrads from breaching his security. (At one point, students were caught using fly rods to cast over the fence and steal buds.) It took ElSohly three years to get DEA permission to grow a strain high in CBD, a nonpsychoactive cannabinoid thought to have many healthful properties. The key ingredient in GW Pharmaceutical’s epilepsy drug, it may have promise as an anti-inflammatory and antipsychotic.
“I am the most restricted person in this country when it comes to production of cannabis and different varieties,” ElSohly says. “In Colorado and Washington or any other state where people don’t have to get any approval from anybody, they just do it. They have the freedom to experiment. I don’t have that freedom. My hands are tied. It’s ridiculous.”
It appears that none of the 25 applications to grow marijuana for purposes of medical research have gone anywhere. (The DEA won’t comment on this or release the names of the applicants.) Craker has yet to get a single call or email about his methods or motivations. No agent has come to inspect his facility or ask questions about security.
He marvels at the power of bureaucratic inertia: “The federal government can be so stubborn. To me they’ve closed their minds.” Craker can’t grow marijuana, but he does lecture about it in his plant medicine classes. “I go through the scenario of what we’ve tried to do,” he says. Ultimately, he says, some of those students may have to do the work he’s been wanting to do for 20 years. “My generation has passed, and we haven’t made it. But it’s going to happen. I just can’t believe it’s going to be forever.”